
How Does Menopause Affect Your Injury Risk as a Runner?
What every female runner in her 40s and 50s needs to understand about bone, tendon, and muscle changes — and how to keep training safely.

If you're a female runner in your 40s or 50s and you've noticed a sudden uptick in niggles, longer recovery times, or injuries that seem to appear out of nowhere — you're not imagining things. And it's not just age.
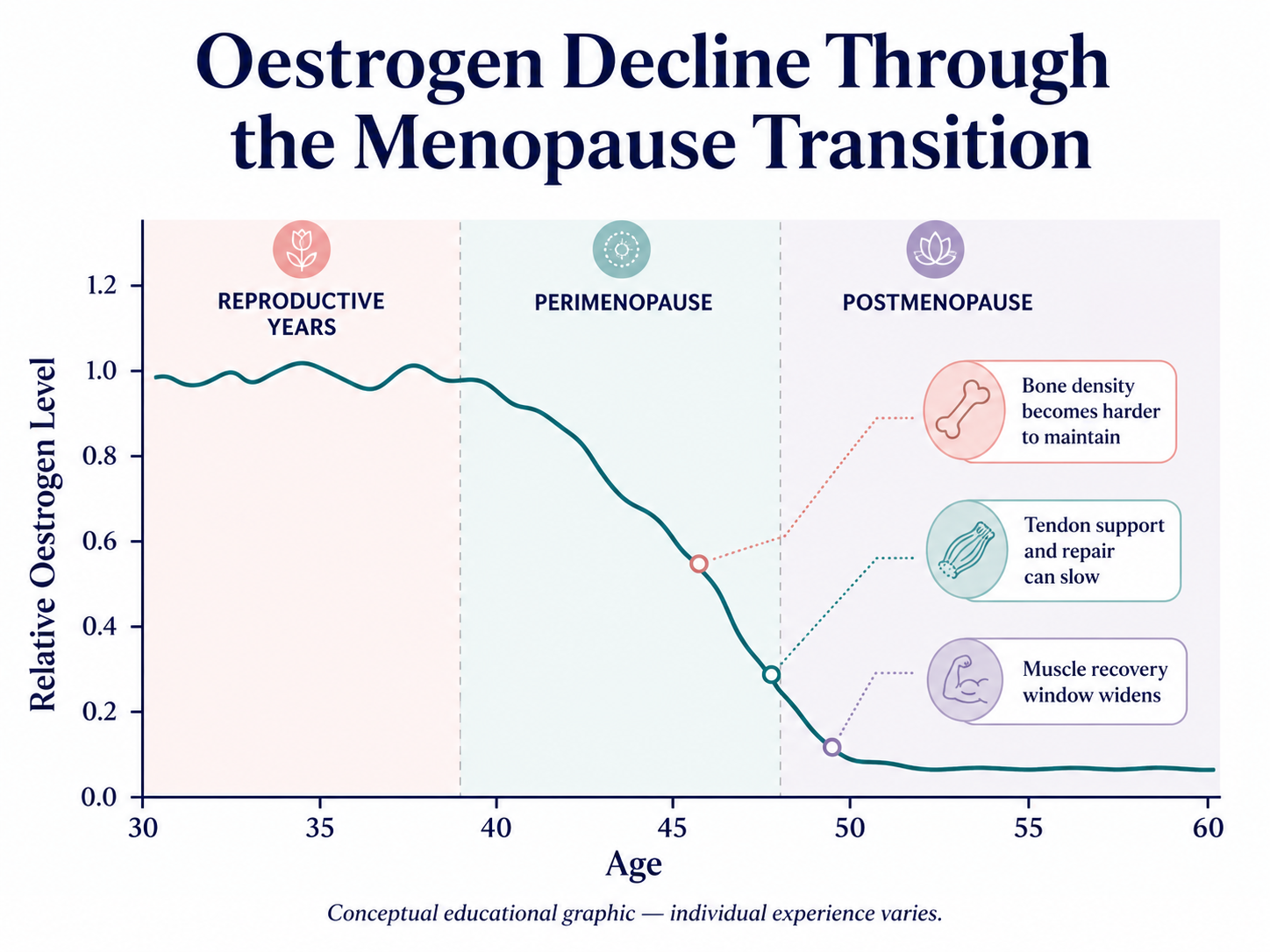
The menopause transition changes the hormonal environment your musculoskeletal system runs on. Oestrogen — a hormone that plays a direct role in bone health, tendon strength, and muscle recovery — declines significantly during perimenopause and menopause. When that happens, your body's ability to absorb training load, repair tissue, and resist injury shifts in ways that most training plans simply aren't designed to account for.
This doesn't mean you have to run less or give up your race goals. But it does mean you need to train smarter, understand what's changing, and know which warning signs to take seriously.
In this article, we break down the three key physiological areas affected by menopause that directly elevate injury risk in runners — bones, tendons, and muscle — and what you can actually do about them.
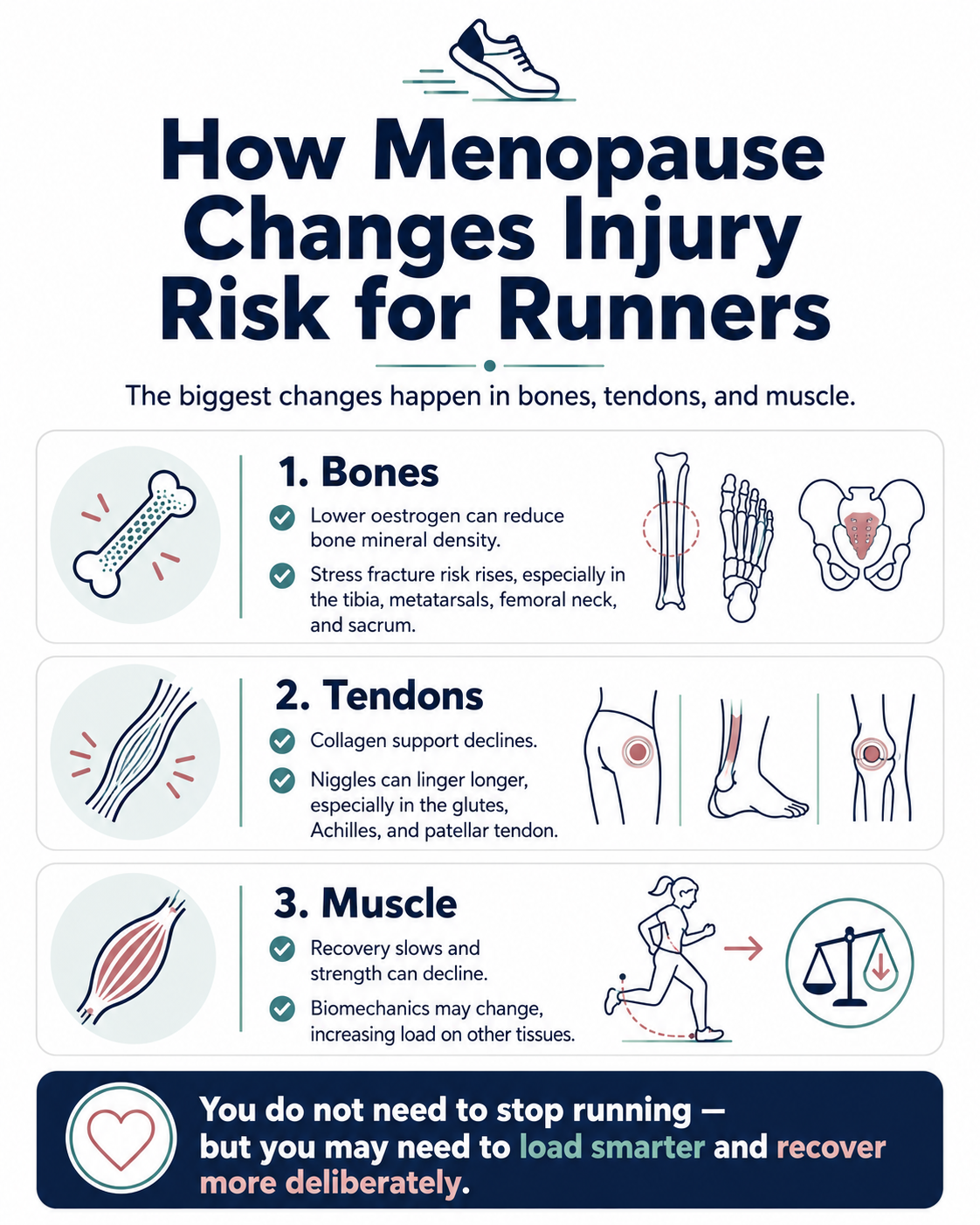
Bones: Why Stress Fracture Risk Increases
Bone health and oestrogen are inseparable. Oestrogen plays a critical role in regulating the balance between bone formation and bone resorption — the constant process by which old bone is broken down and new bone is laid down. When oestrogen declines, the resorption side of that equation accelerates, and bone mineral density (BMD) can decrease more rapidly than at any other point in adult life.
The Endocrine Society notes that the reduction in oestrogen during menopause significantly speeds up bone loss, making menopause the most common underlying cause of osteoporosis. A scoping review published in Frontiers in Reproductive Health (2025) confirms that as oestrogen levels fall during the menopausal transition, bone resorption outpaces bone formation, leading to decreased BMD and elevated fracture risk.
For runners, this matters because the bones most exposed to repetitive impact load — the tibia, metatarsals, femoral neck, and sacrum — are also among the sites most commonly affected by stress fractures.
Lower BMD, Higher Stress Fracture Risk
Research published in Orthopaedic Journal of Sports Medicine followed highly trained female long-distance runners and found that lumbar spine BMD was the strongest individual predictor of whether a runner would sustain a stress fracture within six months. A lumbar spine BMD below 81.1% of the young adult mean was associated with significantly elevated stress fracture risk, with 88% sensitivity.
A separate pilot study in Sports Health found that female runners with a history of stress fractures had measurably lower hip bone mineral density compared to those without, and demonstrated increased bone turnover markers — indicators that bone is breaking down faster than it is being rebuilt.
The Perimenopausal Window
It's important to note that this risk doesn't begin at menopause itself. The perimenopause — the transitional phase that typically begins in the mid-to-late 40s and can last several years — involves fluctuating and declining oestrogen that already starts to affect BMD. Research published in the Journal of Cachexia, Sarcopenia and Muscle confirms that hormonal changes during the menopausal transition, rather than age alone, are the primary driver of bone loss in this life stage.
This means runners who are still having periods but experiencing irregular cycles may already be facing a bone health environment that warrants attention — not just those who have reached full menopause.
What This Means for Your Training
Muscle loss doesn't just affect performance — it affects how your body distributes load during running. Weaker gluteal muscles, for example, alter hip stability and can place disproportionate stress on the knee, Achilles, and iliotibial band. Research on menopause and musculoskeletal health notes that impaired muscle performance contributes to poor balance and increases injury risk — a downstream effect that compounds the direct tendon and bone vulnerabilities described above.
What This Means for Your Training
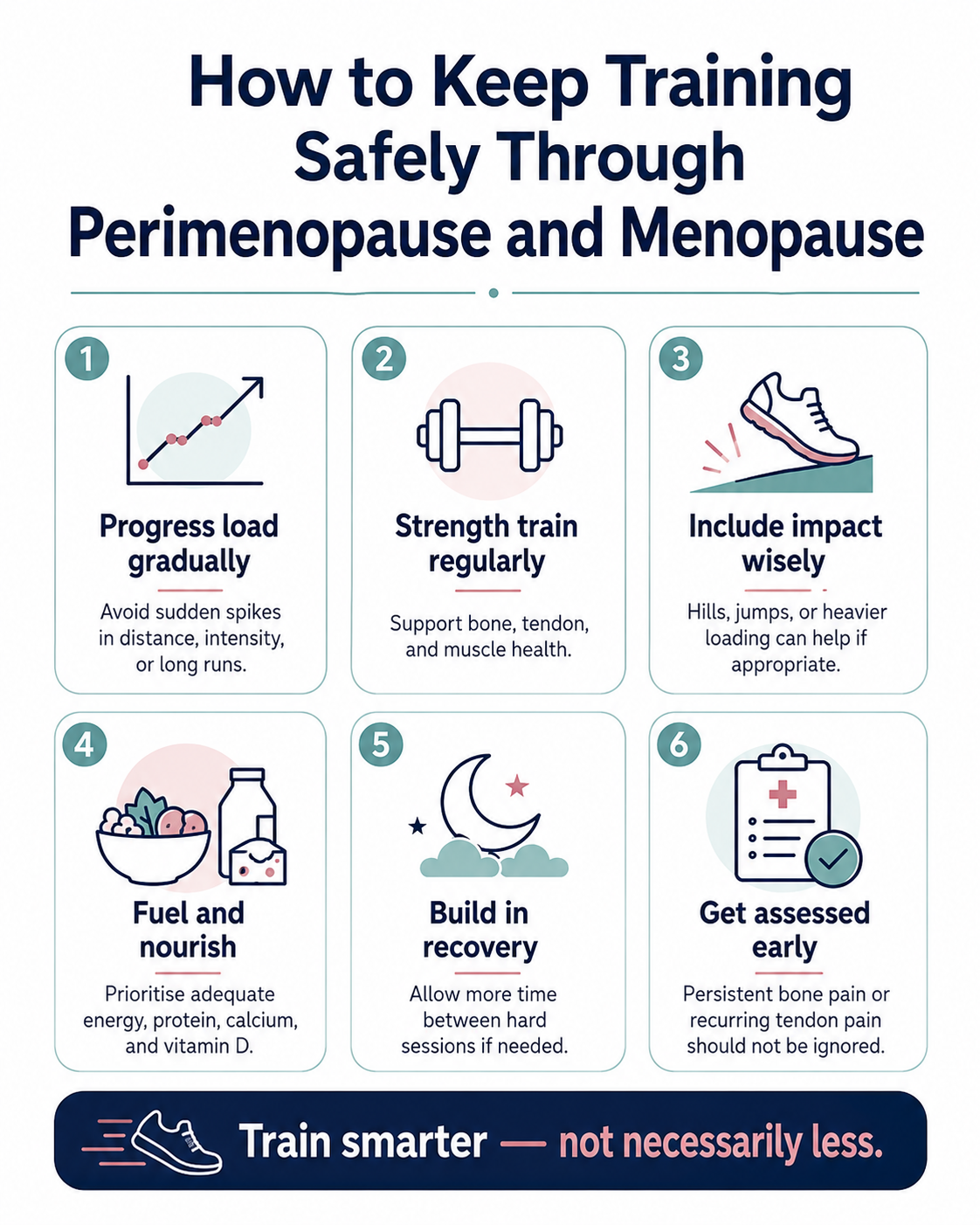
• Training load increases that might have been well-tolerated in your 30s can create stress fracture risk more readily in your 40s and 50s. Gradual load progression is essential.
• Bone density is not something you can feel or easily assess without testing. Any bone-site pain that persists beyond a few days of rest should be evaluated clinically.
• Weight-bearing exercise — including running — does stimulate bone formation and remains one of the most important protective factors for BMD. The goal is not to run less, but to load smarter.
• Supplementation with calcium and vitamin D is commonly recommended to support bone health during this transition — but this falls within the remit of your GP or sports dietitian, not your training plan alone.
Tendons: Collagen Changes and Why Niggles Linger
Tendons are the connective tissue structures that transfer force from muscle to bone with every stride. Like bone, they depend on oestrogen to maintain their structural integrity — and that relationship becomes painfully apparent during menopause.
Oestrogen stimulates collagen synthesis and helps regulate collagen turnover. Collagen is the primary structural protein in tendons, giving them the tensile strength and elasticity needed to handle high-load repetitive activity like running. When oestrogen declines, collagen production slows, tendon repair becomes less efficient, and the tissue becomes less resilient to the micro-damage that accumulates with normal training.
Research published by Total Physio Sydney (2026) drawing on current evidence confirms that postmenopausal women have lower collagen density in tendons, which correlates with higher injury rates and slower recovery.
The Most Commonly Affected Tendons in Runners
The tendons most frequently implicated in menopause-related tendinopathy among runners include:
• Gluteal tendons (gluteus medius in particular), leading to lateral hip pain commonly referred to as gluteal tendinopathy
• Achilles tendon, presenting as posterior heel pain or mid-tendon thickening
• Patella tendon, contributing to anterior knee pain presentations
A clinical review from Dr Alison Grimaldi's practice notes that during the menopausal transition, women often present with Achilles, gluteal, or rotator cuff tendinopathy — sometimes with no clear mechanism of injury. The hormonal environment, rather than a specific training error, is the precipitating factor.
Reduced Tendon Resilience and Prolonged Healing
The problem isn't just that tendons are more susceptible to injury — it's that they take longer to recover once injured. Oestrogen supports blood flow to connective tissue, and its reduction means reduced vascularisation, slower nutrient delivery, and a more persistent inflammatory response post-injury. What might have resolved in two weeks in your 30s can linger for months in a low-oestrogen environment.
Tendinopathy that appears resistant to standard rest-and-load management in a peri or postmenopausal runner may require a longer timeline, modified loading, and a clinical assessment that considers the hormonal context.
What This Means for Your Training
• Load-bearing exercise and progressive strength training can improve tendon resilience even during and after menopause — keeping active is one of the most important things you can do.
• Recovery time between hard sessions matters more than it used to. Tendons are slower to repair, so the window between workouts needs to be wider.
• Acute load spikes — a sudden long run, a race without adequate base training, a big jump in weekly kilometres — are higher risk. More gradual progression is required.
• Any tendon pain that doesn't settle with a few days of reduced load, or that recurs every time you pick training back up, should be assessed by a clinician familiar with menopause and musculoskeletal health.
Muscle: Slower Recovery and Changing Biomechanics
Oestrogen's role in muscle health is less widely discussed than its effects on bone and tendon, but it's equally significant for runners. Oestrogen contributes to muscle protein synthesis, limits post-exercise muscle damage, and helps regulate the inflammatory response to training. When oestrogen declines, several things change simultaneously.
Accelerated Muscle Loss
Sarcopenia — the gradual loss of skeletal muscle mass and strength — is typically associated with older age, but research now makes it clear that menopause accelerates this process for women specifically. A study in The Journal of Physiology following women aged 18 to 80 found a sharp decline in strength beginning in the 40s, driven by the hormonal changes of menopause rather than chronological age alone.
A cross-sectional study published in the Journal of Cachexia, Sarcopenia and Muscle found that muscle and bone losses were directly associated with the menopausal transition, with physical activity — especially higher-level activity — being beneficial for preserving skeletal muscle during this period.
Slower Post-Run Recovery
Oestrogen also plays a protective role in recovery. It helps limit muscle damage, reduce oxidative stress, and speed tissue repair after training. When it declines, the inflammatory response to a hard run can become stronger and more prolonged. A 2020 study published in Frontiers in Physiology found that postmenopausal athletes experienced significantly delayed post-exercise muscle recovery compared to premenopausal women — a direct effect of hormonal changes on exercise adaptation.
If you're finding that your legs feel heavier for longer after a long run, or that you're not bouncing back the way you used to — that's physiology, not weakness. Your recovery window has genuinely widened.
Biomechanical Consequences
Muscle loss doesn't just affect performance — it affects how your body distributes load during running. Weaker gluteal muscles, for example, alter hip stability and can place disproportionate stress on the knee, Achilles, and iliotibial band. Research on menopause and musculoskeletal health notes that impaired muscle performance contributes to poor balance and increases injury risk — a downstream effect that compounds the direct tendon and bone vulnerabilities described above.
What This Means for Your Training
• Strength training is no longer optional — it is a core component of injury prevention for runners in the menopausal transition. Load-bearing strength work preserves the muscle mass that protects joints and tendons.
• Recovery days are a genuine training stimulus, not a sign of undertraining. Scheduling a full rest day after your longest or hardest run is appropriate and evidence-aligned.
• Training by perceived effort, rather than hitting specific pace targets, can help avoid the risk of chronically overloading a body whose adaptation window has shifted.
• Gait analysis can identify whether specific biomechanical changes — such as reduced hip stability or altered foot mechanics — have emerged and are contributing to injury patterns.
How The RunClinic Can Help
Understanding the physiological changes of menopause is one thing. Knowing how they're expressing themselves in your body — and adjusting your training accordingly — is another. That's where a structured assessment can make a real difference.
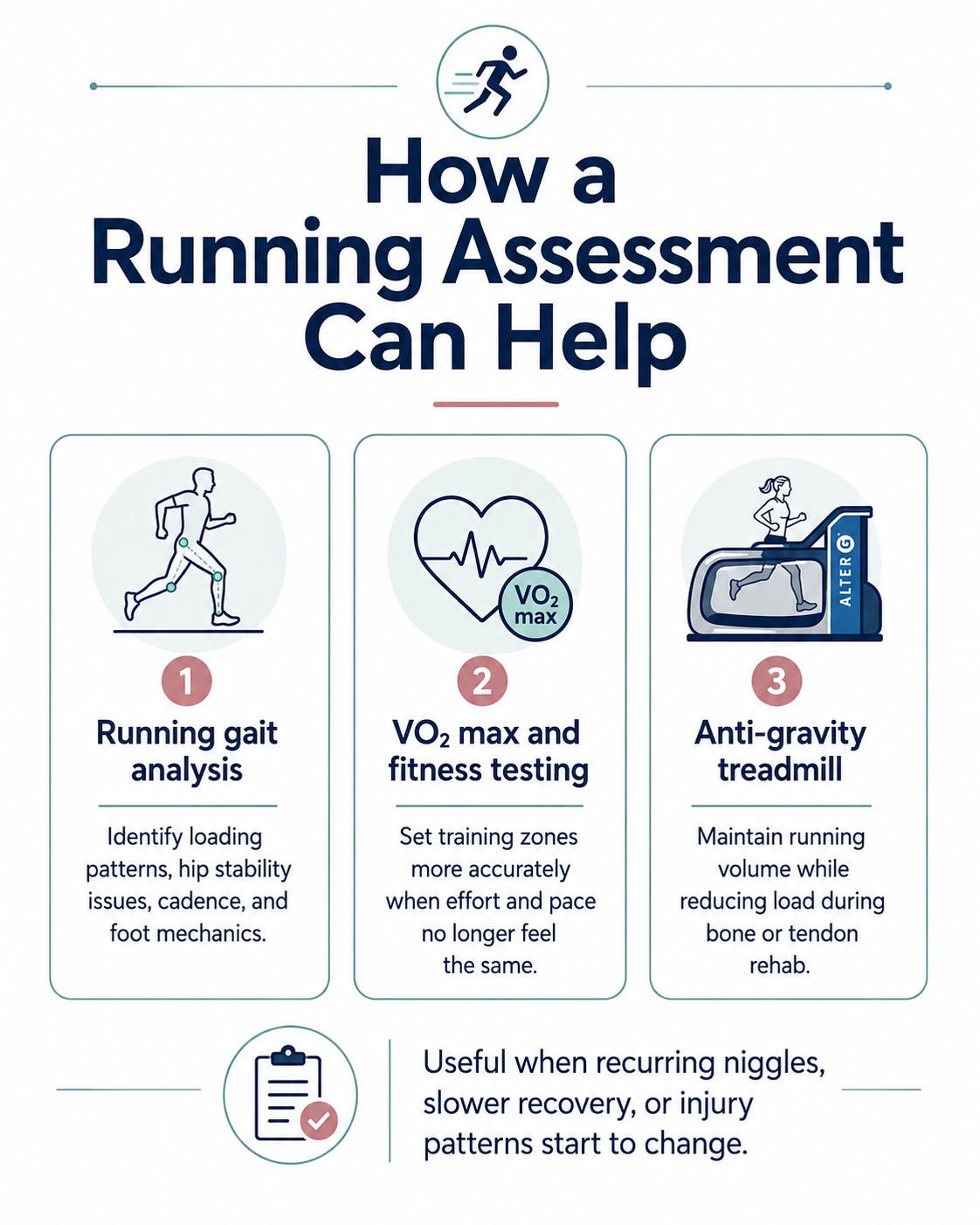
Running Gait Analysis
If you've noticed increased loading on one side, recurring hip or knee pain, or altered stride mechanics, a full gait analysis can identify whether and how menopause-related muscle changes are affecting your running pattern. We assess ground contact time, hip drop, cadence, loading rates, and foot strike mechanics — giving you a precise picture of where your body is under stress.
VO₂ Max and Fitness Testing
Declining muscle mass and altered recovery can affect aerobic capacity and running economy. A VO₂ max assessment gives you an objective measure of your current fitness and can help inform appropriate training zones — particularly important when perceived effort no longer aligns reliably with previous pace-based training targets.
AlterG Anti-Gravity Treadmill
For runners managing bone stress reactions, tendinopathy, or simply trying to maintain volume without overloading healing tissue, the AlterG anti-gravity treadmill allows continued running at a fraction of your body weight. This is particularly valuable during the menopausal transition, where the gap between desired training load and tolerable tissue load may be narrower.
Key Takeaways
Menopause is a genuine musculoskeletal transition for female runners — not a reason to stop, but a reason to train differently. The three primary injury risks are:
• Bones: Reduced BMD increases stress fracture susceptibility, especially at the tibia, metatarsals, and femoral neck.
• Tendons: Declining collagen production makes tendons less resilient and slower to recover from load.
• Muscles: Accelerated muscle loss and prolonged recovery timelines change how the body distributes and absorbs impact forces.
The good news is that running itself remains one of the most protective things you can do for bone density and muscle mass during this transition. The goal is not to do less — it's to load more intelligently, recover more deliberately, and seek clinical guidance when something doesn't settle.
If you're a female runner in your 40s or 50s and you've started accumulating niggles that weren't there before, don't just push through. Get assessed. Understanding your baseline is the first step to training through this transition with confidence.
DISCLAIMER
This blog is for general educational purposes only and does not constitute medical advice or diagnosis. If you are experiencing pain, injury, or symptoms that concern you, please seek assessment from a qualified healthcare professional. For guidance on nutrition, calcium, vitamin D, or hormonal therapies, speak with your GP or a registered sports dietitian.
REFERENCES
1. Endocrine Society. (2022). Menopause and Bone Loss.
2. Saito, T. et al. (2021). Identification of Predictive Risk Factors for Stress Fracture in Highly Trained Female Long-Distance Runners. Orthopaedic Journal of Sports Medicine.
3. Johnston, B. et al. (2020). Physiological Factors of Female Runners With and Without Stress Fracture Histories. Sports Health. PMC7787571
4. Doyle, E.M. et al. (2025). Impact of menopause hormone therapy, exercise, and their combination on bone mineral density. Frontiers in Reproductive Health. 10.3389/frph.2025.1542746
5. Sipila, S. et al. (2020). Muscle and bone mass in middle-aged women: role of menopausal status and physical activity. Journal of Cachexia, Sarcopenia and Muscle.
6. Grimaldi, A. (2025). Menopause and Musculoskeletal Health: Why it matters.
7. Total Physio Sydney / Schneider, M. (2026). Menopause and Tendon Injuries: An Evidence-Based Guide.
8. Rothschild & Collingwood (2023). Cited in Running Physio: Menopause Transition in Athletes.
9. Smith, T. (2020). Postmenopausal athletes and delayed post-exercise muscle recovery. Frontiers in Physiology.
10. Haver, M.C. (n.d.). Menopause and Muscle Loss: Why Sarcopenia Starts Sooner Than We Thought.