
Training through Injury: Your Guide to Alternative Training Options
How to stay fit, maintain fitness, and protect your return to running — even when you can’t run.
Getting injured is one of the most frustrating things that can happen to a runner. One week you’re ticking off solid training sessions, the next you’re sidelined, watching your fitness feel like it’s slipping away. But here’s the truth: being injured doesn’t mean training has to stop it just means you need to get smarter and adapt.
The good news? There are evidence-supported alternatives that can help you maintain aerobic fitness, protect your musculoskeletal health, and set you up for a stronger return to running. This guide breaks down what your options are, what the research actually says, and how to approach each one safely.
Important note: You should always get your injury assessed by a health professional to work out the root cause first .
1. Deep Water Running (Aqua Jogging)

Deep water running (DWR) is one of the most sport-specific alternative training tool available to injured runners. You mimic your natural running gait in a pool while suspended by a flotation belt — completely offloading impact forces. This is a tool I’ve used plenty of times as a junior and not enough people are aware of its benefits. You can essentially replicate any training session that you would do on land whilst completely offloading injured structures.
What the research says
Research published in the Journal of Strength and Conditioning Research has demonstrated that well-trained runners who substituted deep water running for land-based training for up to six weeks maintained their VO2 max and running performance compared to those who continued land training (Dowzer et al., 1998). A review by Wilder & Brennan (1993) in the Archives of Physical Medicine and Rehabilitation also found DWR to be an effective modality for cardiovascular conditioning without musculoskeletal loading. More recently, research suggests DWR preserves running economy and aerobic capacity over short injury periods when training intensity is appropriately maintained.
Best for
• More significant injuries where complete offloading is required
like Stress fractures, bone stress injuries
• Shin splints (medial tibial stress syndrome)
• Plantar fasciitis in acute stages
• Post-surgical recovery
How to use it
Get yourself a flotation vest (from a swimming / rehab shop) that clips around your waste and keeps you buoyant. Run with hands in typical thumb a d index finger light hold and dont scoop with your hands! Let the vest take all the weight and cycle your legs more up and down rather than raking or cycling. You will not progress forward very quickly if doing it correctly, but it’s still bloody hard work! N.B. Replicate your regular running sessions as closely as possible — e.g. long run , fartlek, intervals , threshold including intervals (all based on time and PE). Heart rate runs approximately 10–15 bpm lower in water than on land at equivalent perceived effort, so use rate of perceived exertion (RPE) as your primary guide rather than heart rate alone.
2. Anti-Gravity Treadmill (AlterG / Boost)

The Anti-Gravity treadmill uses differential air pressure technology to reduce your effective body weight during running. You can train at 20–100% of your body weight, allowing you to maintain actual running form and neuromuscular patterns during injury recovery — something very few other modalities can match.
What the research says
Studies published in Physical Therapy in Sport and the Journal of Orthopaedic & Sports Physical Therapy support the use of body-weight-supported treadmill running in rehabilitation settings, noting preserved running kinematics at reduced body weight loads. Research suggests that running gait patterns at 80% body weight closely mirror full body weight running, making AlterG particularly effective for maintaining running-specific neuromuscular conditioning (Grabowski & Kram, 2008). Clinical evidence also supports its use in earlier return-to-run progressions than traditional land-based protocols.
Best for
• Bone stress injuries in subacute/recovery phases
• Achilles tendinopathy management
• Hip and knee load management
• Post-surgical return to running
How to use it
Work with your health professional to determine an appropriate starting body weight percentage for your injury. A graduated progression — typically increasing body weight load week by week as tissue tolerance improves — is the standard approach. The RunClinic offers Antigravity treadmill sessions specifically for injury rehabilitation and return-to-run progression.
3. Cycling (Road, Stationary, or MTB)

Cycling is one of the most accessible and well-researched forms of cross-training for injured runners. It provides a high cardiovascular stimulus with minimal impact loading, making it suitable for a broad range of running-related injuries.
What the research says
Evidence published in the European Journal of Applied Physiology indicates that cycling can maintain aerobic fitness during periods of reduced running training, with other research showing that fitness and performance over 2 miles can be maintained through cross training for up to 6 weeks (if intensity is maintained). Though research suggests cycling and running do share partial cardiovascular transfer but differ in peripheral muscular adaptations (Tanaka, 1994). This means cycling won’t perfectly replicate running fitness, but it will significantly blunt detraining effects on cardiorespiratory capacity over short injury periods.
Best for
• Upper limb injuries (obvious advantage)
• Plantar fasciitis (standard cycling is low-impact on the plantar fascia)
• General lower limb stress injuries where axial loading needs to be reduced
Watch out for
Cycling isn’t always pain-free for runners. Forefoot pathology can sometimes be irritated and Knee issues/ ITB in particular can be aggravated if bike fit isn’t optimal. If you’re cycling through injury, seek the advice of your health professional and a basic bike fit before committing to volume. Also note that high-cadence cycling doesn’t replicate the hip extension demands of running, which can affect hip flexor and glute strength maintenance.
4. Swimming and Pool-Based Training

Swimming provides exceptional cardiovascular conditioning with near-zero impact loading. While it doesn’t mimic the running movement pattern as closely as DWR, it remains an effective tool for maintaining overall aerobic base during injury.
What the research says
Research consistently shows swimming maintains VO2 max and cardiovascular capacity during running injury periods, though due to differences in muscle recruitment patterns and body position, there is limited direct transfer to running economy. A study by Mutoh et al. found that swimming maintained aerobic fitness effectively in injured runners, though sport-specific neuromuscular adaptations were not preserved to the same extent as DWR. Swimming is best viewed as aerobic maintenance rather than running-specific conditioning.
Best for
• Bone stress injuries requiring full offloading
• Lower limb injuries with significant pain on weight-bearing
Athletes who enjoy swimming and / or want active recovery days between DWR or cycling sessions
5. Elliptical Trainer

The elliptical offers a middle ground between cycling and running — a cyclical, lower-limb-dominant movement with some similarities to running gait, but without the impact. It’s widely available, easy to use, and provides a reasonable aerobic stimulus.
What the research says
Research by Mercer et al. (2003) in the Journal of Applied Biomechanics found that elliptical training produced similar muscle activation patterns to running in the major lower limb muscle groups, making it more running-specific than cycling in terms of muscular demands. However, the lack of true flight phase and ground reaction forces means it doesn’t fully replicate running mechanics. Evidence suggests it is effective for maintaining aerobic fitness and can reduce injury-related deconditioning during recovery.
Best for
• Later stage bone stress injuries where shock atenuation is still an issue
• Runners not yet cleared to run but managing hip, knee, or Achilles load
• Early return-to-activity phases where impact needs to be gradual
6. Hiking and Low-Intensity Walking

Hiking and brisk walking don’t get enough credit as training alternatives. Depending on the injury, low-to-moderate intensity walking on varying terrain can maintain some aerobic base, keep the lower limbs active, and — importantly — support your mental health during an injury layoff.
What the research says
Hiking and walking are well-supported in musculoskeletal rehabilitation literature as low-load, functional movement that promotes tissue healing through mechanical loading without high peak forces. For bone stress injuries specifically, progressive loading through walking is often used as the first stage of a graduated return-to-run protocol, based on principles of load management described in Sports Medicine guidelines.
Best for
• Low-grade tendinopathies that respond well to controlled loading
• Bone stress injuries in early to mid recovery phases (terrain-dependent)
• Runners who need active recovery while protecting a sensitive structure
• Ultra and trail runners who need to maintain time-on-feet without running load
A note on hiking load
Downhill hiking in particular places significant eccentric demand on the quads and anterior tibial structures. If you’re managing a shin or knee issue, technical downhill terrain may still be too provocative. Check with your treating clinician.
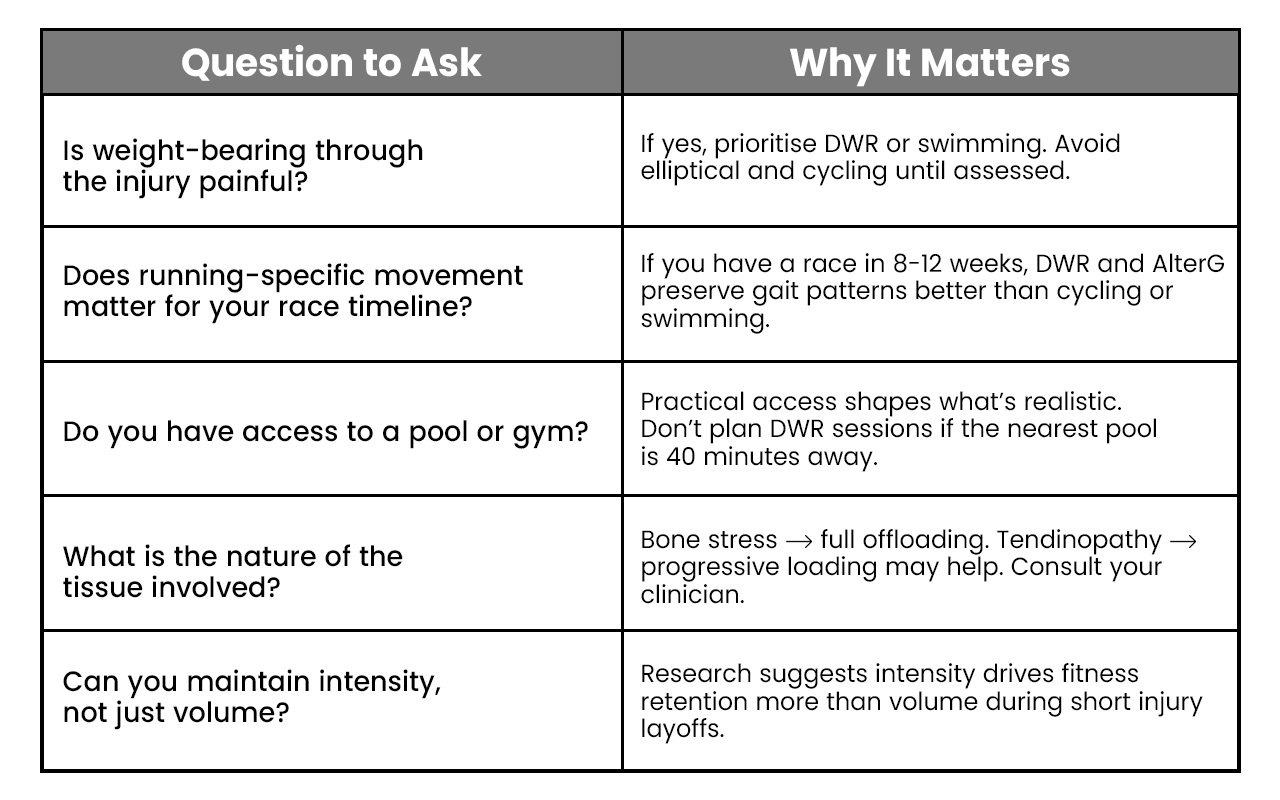
Choosing the Right Option: Key Questions to Ask
Not every alternative works for every injury. Here’s a practical framework:
How Much Fitness Do You Actually Lose?

This is the question every injured runner wants answered. The short version: less than you think, if you act quickly.
Research on detraining (the physiological effects of reduced or ceased training) consistently shows that aerobic capacity begins to decline within 10–14 days of complete inactivity, with more significant losses occurring after 3–4 weeks. However, the rate of detraining is highly dependent on the athlete’s training history — well-trained runners retain fitness longer than beginners (Mujika & Padilla, 2000, Medicine & Science in Sports & Exercise).
The key takeaway: maintaining even 50–70% of your normal training load through cross-training can significantly blunt detraining effects. Intensity appears to be particularly important — research suggests that training intensity preserves aerobic adaptations better than volume during periods of forced reduction.
Translation for runners: doing hard intervals in the pool or on the bike beats doing easy laps at low intensity, even if you’re clocking the same time.
Planning Your Return to Running
Cross-training isn’t just about surviving injury — it’s about setting yourself up for a successful return. That means:
• Maintaining aerobic base so your cardiovascular system isn’t starting from zero
• Keeping neuromuscular patterns as close to running as possible (DWR and AlterG are best here)
• Protecting the injured structure by respecting load — more isn’t always better
• Following a graduated return-to-run protocol as directed by your clinician
At The RunClinic, we use gait analysis and AlterG treadmill sessions to support runners through injury recovery and into a structured return-to-run program. If you’re not sure where to start, that’s exactly the conversation to have with your treating professional.
References & Evidence Base
Dowzer CN, Reilly T, Cable NT. Effects of deep and shallow water running on spinal shrinkage. British Journal of Sports Medicine. 1998;32(1):44-48.
Grabowski AM, Kram R. Effects of velocity and weight support on ground reaction forces and metabolic power during running. Journal of Applied Biomechanics. 2008;24(3):288-297.
Mercer JA, Dufek JS, Bates BT. Analysis of controlled stride length conditions for treadmill and outdoor running. Journal of Applied Biomechanics. 2003;19(4):305-315.
Mujika I, Padilla S. Detraining: loss of training-induced physiological and performance adaptations. Part I: short term insufficient training stimulus. Sports Medicine. 2000;30(2):79-87.
Tanaka H. Effects of cross-training: transfer of training effects on VO2max between cycling, running and swimming. Sports Medicine. 1994;18(5):330-339.
Wilder RP, Brennan DK. Physiological responses to deep water running in athletes. Sports Medicine. 1993;16(6):374-380.
Sports Medicine Australia. Position Statement on Return to Sport. SMA, 2022. Available at: www.sma.org.au
Disclaimer: This content is for educational purposes only and does not constitute medical advice. Always seek guidance from a qualified sports medicine professional, physiotherapist, or podiatrist before commencing any training program, particularly during injury recovery.